Abstract
Background: There is currently a national mental health crisis due to the lack of access to mental health care. Objectives: 1. To study the different factors that contribute to lack of access to psychiatric treatment. 2. To compare each factor by ranking them according to their relevance in contributing to the lack of access to health care and national mental health crisis as perceived by psychiatrist respondents to a brief survey. 3. To analyze results, discuss implications, and provide recommendations. Methods: Seven factors contributing to lack of access to psychiatric treatment are identified from a review of literature, educational materials, and clinical practice. A cross-sectional survey of psychiatrists in US practice is conducted from July to December 2023 by convenient sampling. Recruitment is done in person and via email, US postal mail, and telephone. Forty-eight respondents rated these factors in a Likert scale and ranked them, taking 15 minutes to complete each survey. Quantitative data are analyzed descriptively, and qualitative data are analyzed deductively by identifying the themes from respondents’ narratives. Results: The factors contributing to lack of access to psychiatric treatment are ranked as follows: 1. Lack of support to mental health organizations to establish and operate high-performance mental healthcare delivery (score: 11). 2. Leadership problem and administration problem (score: 12). 3. Stigma in psychiatrists and patients (score: 10) 4. Lack of support in training medical students (score: 9) 5. Disparity in mental healthcare delivery (score: 6) 6. Breakdown of family structure as, “Family is the cradle of good citizenship” (score: 8) 7. Shortage of psychiatrists (score: 6). The theme that emerged from respondents’ narratives about keeping their job are: 1. Enjoyment 2. Financial 3. Altruism 4. Structure. Conclusions: This study has affirmed the relevance of Psychiatry and the need to improve access to mental healthcare. This will require systemic approach from mental health providers to communities, institutions, and healthcare organizations. It is hoped that studies such as this will spark a cultural transformation that will reverse healthcare access issues.
Keywords
Mental Health Crisis, Survey, Accessibility Factors, Psychiatrist Respondents
1. Introduction
"Without mental health, there is no true physical health"
| [1] | Pollack, R. Foreword in Trevedi H., Sharfstein S. Editors. Textbook of hospital psychiatry. 2nd Ed. Washington, DC: American Psychiatric Association Publishing. 2023. p. xix. |
[1]
. Currently, there is a national mental health crisis due to a lack of access to mental healthcare. This accessibility issue to mental healthcare has a significant impact on the most vulnerable minority populations; immigrants
| [2] | Agudo M, Richie W. Panic disorder diagnosed as schizophrenia: a transcultural issue. National Medical Association. 100th Scientific Assembly. Annual Chester M. Pierce, MD, ScD Resident and Medical Student Symposium. 1995 July 31. |
[2]
; racially/ethnically diverse Black, Indigenous, People of Color (BIPOC); women in maternity and perinatal phase
| [3] | Wisner K, Murphy C, Thomas M. Prioritizing maternal mental health in addressing morbidity and mortality. JAMA Psychiatry. 2024; 8l (E2-E6). |
[3]
; older adults
| [4] | Ehassan H, Robbins-Welty G, Moxley J. Geriatric psychiatrists' perspectives on palliative care: results from a national survey. Journal of Geriatric Psychiatry and Neurology. 2024; 37(1): 3-13. |
[4]
; and those who are gender diverse or identify as LGBTQIA+. This vulnerable population includes those who are marginalized
| [2] | Agudo M, Richie W. Panic disorder diagnosed as schizophrenia: a transcultural issue. National Medical Association. 100th Scientific Assembly. Annual Chester M. Pierce, MD, ScD Resident and Medical Student Symposium. 1995 July 31. |
[2]
; those who are incarcerated
| [7] | Wei, L, Woodruff A, et al Comment & response. Opioid use disorder treatment for patients who are incarcerated. JAMA. 2023; 330(13): 1284-5. |
[7]
; and those with complex and chronic debilitating medical conditions
| [4] | Ehassan H, Robbins-Welty G, Moxley J. Geriatric psychiatrists' perspectives on palliative care: results from a national survey. Journal of Geriatric Psychiatry and Neurology. 2024; 37(1): 3-13. |
| [8] | Strawbridge R, Graham N. Editorials. Dissecting the genetic relationship between schizophrenia and cardiovascular disease. Am Journal of Psychiatry. 2023; 180(11): 785-6. |
[4, 8]
For example in migrants, mental distress is greatest in the marginal category and rejection category, and least in the integration category. Intermediate mental distress is found in assimilation and separation categories
| [2] | Agudo M, Richie W. Panic disorder diagnosed as schizophrenia: a transcultural issue. National Medical Association. 100th Scientific Assembly. Annual Chester M. Pierce, MD, ScD Resident and Medical Student Symposium. 1995 July 31. |
[2]
. Please refer to
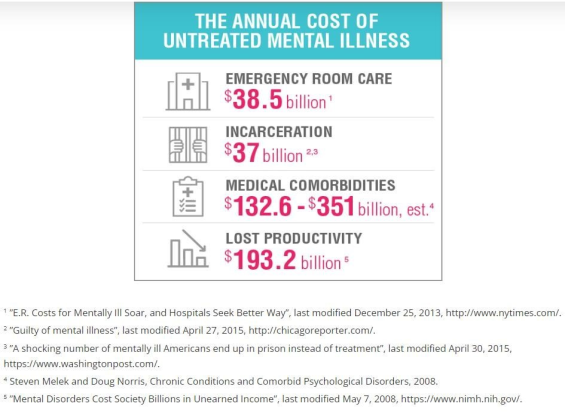
Tables 4 and 5. The chronicity and burden of comorbid mental health disorders within these vulnerable populations directly impact the patients and indirectly impact their families and society in multiple ways. Without prompt and appropriate psychiatric treatment, it leads to their early demise due to suicide, homicide, accidents, unintentional injuries, downward drift phenomenon, treatment-resistant psychiatric, and comorbid medical conditions. The burden and chronicity of unmanaged psychiatric conditions in patients is a challenge for families to remain intact and function in harmony. Due to the patients' lack of productivity, it leads to a reduced workforce and bleak societal economics
| [9] | Martins R, Kadakia A, Williams R, et al. The lifetime burden of schizophrenia as estimated by government-centric fiscal analytic: framework. J Clin Psychiatry. 2023; 84(5): 30-7. |
| [41] | Greenlaw, S, Shapiro D. Principles of Microeconomics. AnnArbor (MI): Rice University OpenStax.2018. p. 83. |
[9, 41]
. As can be seen in
Figure 7 of Appendix IV, the costs of untreated mental illness in the US are estimated to be between $300 billion and $500 billion per year.
According to National Alliance on Mental Illness statistics, individuals in the Veterans Health Administration have a prevalence of 40% of diagnosed mental illness or substance use disorder. The prevalence of major depressive disorder is
9.7%, anxiety disorders 20% bipolar I disorder 2.8%, and schizophrenia, 1.19%. Patients diagnosed with schizophrenia are estimated to have an annual fiscal burden in the US of $173.6 billion and the lifetime fiscal loss to the government per person is $1,540,042. According to the Centers for Disease Control and Prevention, suicide is a leading cause of death in the U.S. with 45,979 deaths in the U.S.
| [5] | Redd, K. "Suicide is a public health crisis". Native Americans disproportionately impacted by suicide. ABC lo+. 2023 March 24. |
[5]
. Native Americans and their communities are disproportionately impacted by suicide
| [5] | Redd, K. "Suicide is a public health crisis". Native Americans disproportionately impacted by suicide. ABC lo+. 2023 March 24. |
| [6] | Weinstock, C. Native American communities have the highest suicide rates, yet interventions are scarce. CNN KFF Health News. 2024, January 26. |
[5, 6].
In the years between 2019 and 2020, suicide rates increased by 6% among Native Americans and by 4% among Blacks. There was a 4% decrease in suicide rates among the Whites. The prevalence of suicidality is 17.2% among high school students, and 47.7% of LGBTQ youth express suicidality
| [10] | Moukaddam, N. What happens to your psychiatric patient beyond the emergency department. Audio Digest. 2022 Sept 21; 51(18). |
[10]
. Adverse childhood experiences (ACE) are associated with earlier instances of substance use
| [11] | Meadows A, Strickland J, Haeder S. et al. Adverse childhood experiences and early initiation of substance use: A survival analysis. The International Journal of Psychiatry in Medicine. 2024; 59(2): 218-31. |
[11]
. The youth have difficulty achieving their educational goals and suffer from identity crisis. Healthcare policies are formulated in an attempt to reduce distress and suffering, but some are controversial and cause opposition and division in the community (i.e., euthanasia
| [12] | Yatgur, B. Euthanasia for mental illness: right or wrong. Clinical Psychiatric News. 2023; 51(11): l. |
[12]
, abortion, in-vitro fertilization, rationing of healthcare benefits for the elderly, and disparity
| [13] | Levounis P. In confronting addiction, older adults fall through the cracks. From the president. Psychiatric News. 2023; 58(10): 2. |
| [14] | Moran M. Levounis convenes medical leaders to collaborate on addiction. Psychiatric News. 2023; 58(10): l. |
| [15] | Ortega A., Roby D. Ending structural racism: US healthcare System to eliminate healthcare inequities. Department of Health Public Policy. JAMA 2021; 326(7): 613-15. |
| [16] | Mensah M, Owda D, Simons E, et al. Research letter US postgraduate trainee racial, ethnic, gender representation and faculty compensation by specialty. JAMA. 2023; 330(9): 872. |
[13-16]
in healthcare).
For the most part, we, as psychiatrists, have our focus solely on the patients, but just as with the dyadic relationship mother-infant dynamics of psychopathology, child psychiatrists look at the wellbeing and strength of the mother to accomplish her task to influence the health of her infant. In this analogy, I shift the focus on the psychiatrist-patient dyadic relationship wherein mental health providers and intricate mental healthcare systems influence patient treatment outcomes and the current state of national mental health.
Lack of access to mental healthcare has been in existence chronically, but it is further aggravated by the COVID-19 pandemic, an acute-on-chronic problem that is considered "syndemic"
| [17] | Da Silva F. Carvalho 0, Neto R. "COVID-19 and immunization: Reflections and rationale on why child and adolescent psychiatry should help. JMCAP. 2023; 62(5): 509- 11. |
[17]
due to simultaneous emergence of multiple epidemic problems. The US mental healthcare issue is also manifested worldwide as mental health gap
| [18] | Brohan H, Chawdhary N, Dua T. The WHO Mental Health Gap Action Programme for mental, neurological, and substance use conditions: the new and updated guideline recommendations. The Lancet. 2023; 11: 155-58. |
[18]
. Psychiatric treatment spans from the realm of prevention, treatment of the mental disorder, and finally to recovery
| [13] | Levounis P. In confronting addiction, older adults fall through the cracks. From the president. Psychiatric News. 2023; 58(10): 2. |
| [14] | Moran M. Levounis convenes medical leaders to collaborate on addiction. Psychiatric News. 2023; 58(10): l. |
[13, 14]
at all human life ages.
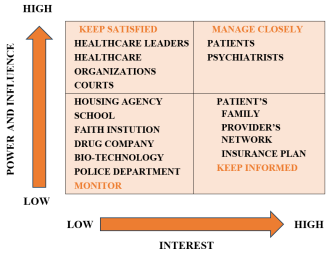
Focusing on who are the key players in healthcare, please refer to the standard stakeholder grid chart
| [44] | Austin J, Bentkover J, Chait L. Leading strategic change in anera of healthcare transformation. Providence (RI): Springer International Publishing Switzerland. 2016. p. 61. |
[44]
in
Figure 1. Looking at the top-right quadrant, both patients and psychiatrists need to be managed closely because these stakeholders have high levels of both power/influence and interest. They need ongoing focus and communication.
At the top-left quadrant, healthcare organizations, healthcare leaders, and courts have high power and influence, but their level of interest is lower. These stakeholders need to be kept satisfied over time, and in some cases, helped to develop stronger interest so that they can be additional advocates of improvements in mental-health access.
The stakeholders at the bottom-right quadrant (patients' families, psychiatrist providers' network, and insurance plan) have a high level of interest, but much lower power and influence. They simply need to be kept informed.
The stakeholders at the bottom-left quadrant (housing agency, school, faith institution, drug company, bio-technology, innovation, and police department) have low levels of power/influence and interest related to the issue of mental-health access, so they simply need to be monitored to see if their positions in the grid change.
Finally, plausible scenarios that each stakeholder can shift to a different grid should be envisioned, especially with the change of healthcare landscape. For example, insurance plan which needs to be kept informed can acquire so much power and influence that would rightly fall at the top-right quadrant to be managed closely.
2. Objectives
The objectives of this study are:
1. To study the different factors that contribute to lack of access to psychiatric healthcare and the national mental health crisis.
2. To compare the factors by ranking them according to their relevance as perceived by psychiatrists who responded to a brief survey.
3. To analyze results, discuss implications, and provide recommendations.
It is hoped that this study can contribute to the solution of the above problems by offering clear perspectives on the topic of mental healthcare. The goal is that this overarching perspective will provide a segue way for further research, ideas, and policies to improve patients' well-being and to educate the public.
3. Methods
A cross-sectional, seven-item factors, questionnaire survey was offered to psychiatrists from July 2023 to December 2023. Psychiatrists' names were obtained via convenience sampling through in-person, email, US postal mail, and telephone. A mixed-method study approach incorporating both qualitative and quantitative aspects was utilized. The setting of the research project includes US psychiatric practices (particularly residency and fellowship institutions), listservs of psychiatric organizations, psychiatric conferences, state board medicines websites, and other mental-health entities. For ease of conceptualization, the tabulation of the results and figures is found in Appendix I.
The seven factors are identified and derived from a review of literature, educational materials, and clinical practice. The factors are identified and rated on a grid scale and are ranked by the respondents. The survey requested that respondents utilize a Likert-scale rating for each factor: (5) completely agree, (4) partially agree, (3) neutral, (2) partially disagree, and (1) completely disagree. The seven factors are:
1. Lack of support to mental health organizations to establish and operate high- performance mental healthcare delivery.
2. Leadership problems or administration problems in mental health organizations.
3. Shortage of psychiatrists
| [28] | Hallett E, Simeon E, Amba V, et al. Factors influencing turnover and attrition in the public behavioral health system workforce: qualitative study. Psychiatric Services. 2024; 75(1): 55-63. |
[28]
.
4. Stigma in psychiatry and patients with mental illness
| [21] | Maximo S. A scoping review of ethical consideration in spiritua1/religious counseling and psychotherapy. Journal of Pastoral Care & Counseling. 2019; 73(2): 123-133. |
| [35] | Knaak S, Mantler E. Mental illness-related stigma in healthcare: barriers to access and care and evidenced based solutions. Healthcare Management Forum. 2017; 30: 111-6. |
[21, 35]
.
5. Lack of support in training medical students
| [34] | Mercado, A, Boyd J, Chesky K. US medical student health insurance coverage for mental health treatment after the COVID 19 pandemic. JAMA Intern Med 2023; 183(11): 1273- 75. |
[34]
.
6. Breakdown of family structures
| [26] | Luca, M. The two-parent privilege review: where have all good men gone? The Wall Street Journal. 2023 Sept 24. |
| [27] | McMillan K. I survived the foster care system. Dismantling it altogether is the only path forward. USA Today. 2023 Sept 24. |
[26, 27]
: Family is the, "Cradle of good citizenship."
| [29] | Abduhakimovna S. Social-psychological characteristics of the formation of family relations in adolescents. Journal of Child Psychology and Psychiatry. 2024; 7(1): 55-60. |
[29].
7. Disparity in mental healthcare delivery
| [13] | Levounis P. In confronting addiction, older adults fall through the cracks. From the president. Psychiatric News. 2023; 58(10): 2. |
| [14] | Moran M. Levounis convenes medical leaders to collaborate on addiction. Psychiatric News. 2023; 58(10): l. |
| [15] | Ortega A., Roby D. Ending structural racism: US healthcare System to eliminate healthcare inequities. Department of Health Public Policy. JAMA 2021; 326(7): 613-15. |
| [16] | Mensah M, Owda D, Simons E, et al. Research letter US postgraduate trainee racial, ethnic, gender representation and faculty compensation by specialty. JAMA. 2023; 330(9): 872. |
| [23] | Romanelli R; Marjanovick S. Diversity, equity, and inclusion in healthcare innovation: considerations for future research, policy and practice. Rand Corporation Blog. 2022 July 6. |
| [32] | Ruiz-White I, Kramer L, Philips L. et al. Racial and ethnic disparities in physical and mental healthcare and clinical trials. J Clin Psychiatry. 2023; 84(4): 54-64. |
| [33] | Van der Ven E, Susser E. Structural racism and risk of schizophrenia. Am J Psychiatry. 2023; 180(11): 782-4. |
[13-16, 23, 32, 33]
.
An open-ended, qualitative portion of the survey allowed the respondents to reflect on the factors that caused them to remain in their psychiatric practices and career field. The data were analyzed according to frequency and percentages. The questionnaire used is found in
Figure 4 and Figure 5 of Appendix II. A poster for this research is illustrated in
Figure 6 of Appendix III.
4. Results
Considering that this was a mixed-method study, the first part will describe quantitative results and the second part will discuss the qualitative results. There were 50 survey responses, but two were duplicated by the same psychiatrists, reducing the analytic sample to 48 responses. The demographic characteristics of the respondents were also considered but de-identified and reported in aggregate as percentages in
Table 1 of Appendix I. Many of the respondents fall into the 65-69 age bracket (19%), followed by the 55-57 age bracket (17%). The oldest respondent is 85 years of age, and the youngest respondent is 34 years of age. Most of the respondents have between 25-29 years of psychiatric service (20%). The survey respondents were evenly distributed between males and female.
For factor (1) "Lack of support to mental health organizations," the largest group of respondents partially agreed (44%), followed by those who completely agreed (29%). For factor (2) "Leadership problem or administration problem," the results were distributed differently, with the largest group of respondents selecting partially agree (35%), followed by those who chose neutral (21%). For factor (3) "Shortage of psychiatrists," the largest group of respondents chose completely agree (35%), followed by those who partially agree (22%). For factor (4) "Stigma in psychiatry and patients with mental illness," the majority of the respondents partially agree (52%), followed by those who chose completely agree (23%). For factor (5) "Lack of support in training medical students, psychiatry residents, and psychiatry fellows," the largest group of respondents partially agreed (46%) followed by those who chose neutral (21%). For factor (6) "Breakdown of family structure as, 'Family is the cradle of good citizenship,"' the largest group of respondents partially agreed (23%), followed by those who chose neutral (21%). For factor (7) "Disparity in mental health," the majority of the respondents completely agreed 56%, followed by those who partially agreed 27%. These results can be seen in
Table 2 of Appendix I.
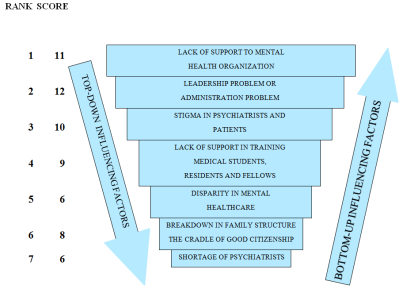
The respondents ranked the seven factors according to their perceived relevance in contributing to the national mental-health crisis. Initial findings reveal a tie between four factors, all of which scored 11. These include factors (1) Lack of support to mental health organizations, (3) Shortage of psychiatrists, (6) Breakdown of family structure as, "Family is the cradle of good citizenship," and (7) Disparity in mental healthcare delivery. A tiebreaker was needed to distinguish between factors (1) and (2), as both have the same score of 12 in the second rank. Factor (1) was given the highest level in rank #1 because it has the highest scores in rank #1 and rank #2. Factor (2) earned the rank# 2. The rankings can be seen in
Table 3 of Appendix I. The final ranking of the seven factors is as follows, with rank #1 as the most relevant factor contributing to the national mental health crisis to rank #7 as the least relevant factor. Please see
Figure 3 of Appendix I.
1. Rank #1. Item factor 1, Lack of support to mental health organizations
2. Rank #2. Item factor 2, Leadership problem or administration problem
3. Rank #3. Item factor 4, Stigma in psychiatrists and patients
4. Rank #4. Item factor 5, Lack of support in training medical students, residents, and fellows
5. Rank #5. Item factor 7, Disparity in mental healthcare
6. Rank #6. Item factor 6, Breakdown of family structure as, "Family is the cradle of good citizenship."
7. Rank #7. Item factor 3, Shortage of psychiatrists
One open-ended question asked, "What is your primary motivation to keep your psychiatry job?" The respondents' narrative statements were noted, and from these, four themes were identified. These include 1. Enjoyment 2. Financial 3. Altruism 4. Structure. These are illustrated in
Figure 2 of Appendix I. Responses to another open-ended question requesting comments/insights/opinions are incorporated in the discussion.
5. Discussions
In the literature review, no studies were found comparing the seven factors contributing to the national mental health crisis from lack of access to mental healthcare through the lens of psychiatrist respondents. It is noted the most prevalent group of respondents was the 65-69 age bracket (19%), followed by the 55-90 age bracket (17%). Thus, the majority of respondents are in the Baby Boomer generation. The years of practice in psychiatric service was revealed to be 25 to 29 years of service among the respondents. Their primary motivation to keep their psychiatric job is illustrated in
Figure 2 and four themes were identified as enjoyment, financial, altruism, and structure.
The number-one ranked factor is the lack of support to mental health organizations. This may be partly due to the high cost of mental healthcare, especially maintaining acute inpatient units, hospitals, or behavioral centers which require several highly specialized professional employees to perform as a team aimed at delivering high-performance psychiatric treatment. In addition, an integrated multimodal approach is essential in running an acute inpatient psychiatric facility, requiring adequate staffing of psychiatric nurses, psychotherapists, occupational therapists, art therapists, music therapists, psychiatric technicians, case managers, internal medicine doctors, pediatricians, and teams of psychiatrists. With changes in the healthcare landscape through acquisitions and mergers, there is a shift from hospital inpatient treatment to lower levels of care such as day hospital programs, intensive outpatient programs, and outpatient clinic settings. The treatment barrier to acute psychiatric hospitals has become very high, while at the same time, there is a long waiting list in most outpatient clinics to accept new intakes. A psychiatrist respondent gave her comment/insight/opinion as follows:
"I believe, in part, the mental health crisis is due to a breakdown of American health system. Insurance companies do not reimburse or pay for psychiatrists to have meaningful and thoughtful visits with their patients. Instead, insurance reimburses for quantity not quality. Psychiatrist and patient burnout become compounded, and we are not the only doctors/people who feel this way."
Psychiatrists do realize acute psychiatric hospitalization is still much needed, especially in the first psychotic break in youths
| [31] | Forsyth J, Bearden C. Rethinking the first episode of schizophrenia: identifying convergent mechanisms during development and moving toward prediction. AJP. 2023; 180(11): 792-804. |
[31]
who need prompt and timely initiation of psychiatric treatment to achieve immediate recovery and prevent chronic sequelae. Emergency situations such as suicide attempts, dangerousness to others, or inability to care for oneself need the therapeutic milieu of hospital psychiatry. Mental health entities or organizations must find the unmet needs of their patients or clients, first-line health care providers, and their administration leaders. With the right spirit, empathy, active listening, observing, and laboring enough to obtain and integrate information from the bottom-up, the goal is to provide support to mental healthcare services that are very much aligned with the needs of the users of the services
| [22] | Kanter R. Why innovation is so hard in healthcare and how to do it anyway. Harvard Business Press. 2011 Feb 22. |
| [25] | Warshay, D. Chapter 3 Step 1 See: find and validate unmet needs. See, solve, scale: how anyone can turn an unsolved problem through success. 2022. |
[22, 25]
.
The Quadruple Aim
| [36] | Khushalani S. Lean and Operational Excellence. Chapter 22 in Trevedi H, Sharfstein S, Editors. Textbook of Hospital Psychiatry. 2nd Ed. Washington, DC. American Psychiatric Association Publishing. c. 2023. p 505. |
[36]
, which is the guiding light for many healthcare organizations to achieve high-performance mental healthcare delivery, would improve the work-life balance of psychiatrists and mental healthcare providers, improve patient experience, improve population health, and reduce healthcare costs.
The factor whose relevance ranked second is leadership and administration problems. The administration has to employ leaders in their healthcare organizations who are endowed with good intrapersonal characteristics and with knowledge, skills, and abilities
| [19] | Cullen-Lester K, Maupin C, Carter D. Incorporating social networks into leadership development: a conceptual mode and evaluation of research and practice. The Leadership Quarterly. 2016; 28(1): 130-52. |
| [20] | Nayar V Employees First/Customers Second: Turning conventional leadership upside down. Harvard Business Press. 2010. |
[19, 20]
. Interpersonal characteristics are essential, especially having refined qualities of confident humility, moral authority, psychological safety, and watchful vigilance for internal scanning and external scanning of risks, threats, and opportunities. Leaders must assume the role of "change champions" to create positive cultural change in their organizations. Good healthcare leaders are familiar with finance and accounting, economics, health law, utilization and management, healthcare marketing, effective communication, and partnerships. They support networking that is open, diverse, and deep in promoting integration and solidarity in the health organization. Employers must be mindful of Employee First/Customer Second (EFCS)
| [20] | Nayar V Employees First/Customers Second: Turning conventional leadership upside down. Harvard Business Press. 2010. |
[20]
.
The third relevant factor is the stigma in Psychiatry as a medical field amongst other medical specialties
| [21] | Maximo S. A scoping review of ethical consideration in spiritua1/religious counseling and psychotherapy. Journal of Pastoral Care & Counseling. 2019; 73(2): 123-133. |
[21]
. In a broader sense, the patients themselves are also stigmatized
| [35] | Knaak S, Mantler E. Mental illness-related stigma in healthcare: barriers to access and care and evidenced based solutions. Healthcare Management Forum. 2017; 30: 111-6. |
[35]
intrapersonally, interpersonally, and socially. The portrayal of mental illness in movies has its pros and cons. It can increase cultural sensitivity, raise awareness, or worsen stigma and instill fear. Many psychiatric units are situated in very remote areas of general hospitals and are the least prioritized for structural improvements. The patients feel the stigma, and their families feel the stigma as well. One psychiatrist respondent remarked:
"There is continued stigma in Psychiatry, and the patients feel these in receiving care due to their mental health diagnosis. Hopefully, there is normalizing of the disparity in mental health delivery. More support is necessary for mental health and substance use disorders."
The fourth-ranked factor is lack of support in training medical students, residents, and fellows. It used to be that medical students had the notion that they should not reveal their mental health needs as this was equated to weakness by their superiors. In addition, licensing boards require physicians to have no prior history of mental illness. Medical students also have inadequate health insurance coverage
| [34] | Mercado, A, Boyd J, Chesky K. US medical student health insurance coverage for mental health treatment after the COVID 19 pandemic. JAMA Intern Med 2023; 183(11): 1273- 75. |
[34]
for mental health care. Some do not have the option to seek psychiatric providers outside of their educational institution and so confidentiality and treatment efficacy are sacrificed. Psychiatric trainees from the global majority must be encouraged and supported to promote inclusion, equity and diversity and promote resiliency within their patient population.
The fifth-ranked factor is disparity in psychiatric healthcare delivery. Discrimination toward the Black, Indigenous, and People of Color (BIPOC) populations compared with the White Population has contributed to racial and ethnic disparities in healthcare. Overdiagnosis or diagnostic bias of Black people for non-affective psychosis appears to have limited measured data in the U.S.
| [2] | Agudo M, Richie W. Panic disorder diagnosed as schizophrenia: a transcultural issue. National Medical Association. 100th Scientific Assembly. Annual Chester M. Pierce, MD, ScD Resident and Medical Student Symposium. 1995 July 31. |
[2]
. Patients who have persistent symptoms and frequent hospital admissions experienced feeling mistreated and unwelcomed by hospital staff. These patients are usually characterized by social determinants of health
| [14] | Moran M. Levounis convenes medical leaders to collaborate on addiction. Psychiatric News. 2023; 58(10): l. |
[14]
that include poor education, poverty, food insecurity, lack of social support, poor living conditions, and poor infrastructures-all of which are drivers of health disparities that pose risk factors for mental health illness. The only recourse for these patients is to seek support in acute psychiatric inpatient facilities, which often results in frequent hospital admissions. There is a great need to implement practices that promote diversity, equity
| [39] | Bai G, Simon K, Cram P. Health equity measures and hospital rankings. JAMA. 2023; 329(9): 764. |
[39]
, and inclusion
| [23] | Romanelli R; Marjanovick S. Diversity, equity, and inclusion in healthcare innovation: considerations for future research, policy and practice. Rand Corporation Blog. 2022 July 6. |
[23]
in mental healthcare to mitigate behavioral and cognitive biases and improve healthcare access.
The sixth-ranked factor is the breakdown of family structure. This is second to the least relevant factor, likely because it is beyond the control of the treating psychiatrist's utilization of their treatment armamentarium. The single-parent household has increased, and the two-parent household has become "household privilege." Fragmented families exist across all socioeconomic strata. It is a sensitive topic to discuss, but certainly, personality development occurs first within the institution of family as the first teaching social container where love, nurturance, and protection are safeguarded
| [24] | Natterson-Horowitz, B. What scientists are learning about women's health from female animals. Scientific American. 2023 March. |
| [26] | Luca, M. The two-parent privilege review: where have all good men gone? The Wall Street Journal. 2023 Sept 24. |
| [27] | McMillan K. I survived the foster care system. Dismantling it altogether is the only path forward. USA Today. 2023 Sept 24. |
[24, 26, 27]
. The mother in the mother-infant dyad dynamic needs to be supported, strengthened, and protected to help her accomplish her task to influence and safeguard the health and wellbeing of her infant. There is a need to improve maternal health in preconception, during the pregnancy period, and during the postpartum period by placing emphasis on the fact that early childhood wellbeing is a critical period of human development
| [24] | Natterson-Horowitz, B. What scientists are learning about women's health from female animals. Scientific American. 2023 March. |
| [38] | Fawzi W, Partap U. Optimizing interventions from early development. JAMA. 2024; 331(1). |
[24, 38].
Improving developmental outcomes of children is the goal, and if this is curtailed right at the very beginning of human development, it follows there is less human capital, low economic productivity, vicious intergenerational cycles of poverty, and poor population health and well being. In other words, ensuring improved developmental outcomes for children will support the propagation of the human species. The presence of fathers
| [26] | Luca, M. The two-parent privilege review: where have all good men gone? The Wall Street Journal. 2023 Sept 24. |
| [30] | Fagan J. The myth oflow-income black fathers' absence from the lives of adolescents. Journal of Family Issues. 2024; 45(1): 144-162. |
[26, 30]
in the family structure is important; they need to be greatly supported, especially when they are faced with challenges such as the phenomenon of "male drift"
| [26] | Luca, M. The two-parent privilege review: where have all good men gone? The Wall Street Journal. 2023 Sept 24. |
[26]
. Family has the primary goal to provide support, protection, monitoring, encouragement, growth with a well-balanced connection and autonomy. Extensive social pressures and challenges can exhaust the strengths of families with extreme pathological reactions of enmeshment, rigidity, coercion, punishment, detachment, and isolation
| [43] | Sharma N, Sargent J. Chapter 9 in Parekh R, Al-Mateen C, Lisotto M et al Editors. Cultural psychiatry with children, adolescents, and families. Washington (DC): First Edition. American Psychiatric Association Publishing. 2021. pp 151-152. |
[43]
. One psychiatrist respondent on the comments/insights/opinions on families, stated, "It may be different for different populations."
Another psychiatrist respondent opined:
"Disintegration of the family unit is detrimental to a person’s mental health. The family of origin is the basic foundation of a child s biopsychosocial development."
The shortage of psychiatrists was ranked last, seventh, by the respondents. Despite the common notion that there is fast turnover of US physicians due to burnout
| [37] | Brady K, Ni P, Lindsey P. et al. Establishing crosswalks between measures of burnout in US Physicians. Gen Internal Med. 2022; 37(4): 777-84. |
| [40] | Young A, Pei X, Arnhart K, et al. FSMB Census of licensed physicians in the United States, 2022. Journal of Medical Regulation. 2023; 109(2): 13-20. |
| [42] | Bullepalli H, Evans R, Ludford S, et al. Burnout among surgeons: lessons for psychiatrists. Current Psychiatry. 2023; 22(8): 23-35. |
[37, 40, 42]
, it appears that from this sample, the majority of the psychiatrists are baby boomers, and they are still actively involved in their profession. One can tell from their narratives in the qualitative data that they have strong reasons to remain involved. There have been gaps in "passing the baton" to early career psychiatrists. Good leadership and mentorship form true collegial relationships for the mentor-mentee with good modelling. Leadership and mentorship provide the opportunity to dispel gaps, behavioral biases, and cognitive biases and to promote the practice of psychiatry.
6. Limitations
This study is cross-sectional, self-funded, and time limited for 6 months. It has a small sample size, recruited by convenient sampling with potential bias. It is a descriptive study conducted by an individual-solo MHL student of Brown University.
7. Recommendations
As a recommendation for future scientific research, a grant-funded follow-up study on a much larger sample size would be in order. It should feature a longitudinal research design, random sampling devoid of bias, and adequate utilization of qualitative and quantitative techniques of data gathering and interpretation. Such a study would bring forth reliable information and educational advancement to psychiatry and promote national mental health wellbeing. With better and more compelling information, policy makers will be in a position to formulate socially just and inclusive policies geared to solving the mental health crisis.
Support is needed:
1. To help mental health organizations reclaim their stability, to encourage the startup of small mental health entities, and to develop a true partnership between the public and private sectors.
2. To support healthcare leaders and those in administration by granting them good, updated educations, better metrics, and better systems. The goal should be to keep them abreast, engaged, and motivated, especially because they have the futures of their patients in their hands.
3. To raise awareness of the need to reduce patient stigma, and to enhance patients' experience of belonging, appreciation, and acceptance.
4. To help educational institutions in the training of medical students, residents, fellows, mentors, and mentees, especially medical students coming from minority groups.
5. To eliminate disparities in mental healthcare.
6. To provide every family with good and affordable health insurance coverage for children, resources for single-parent households, adequate rehabilitation for incarcerated fathers (including eventual reunification with their families), and adequate protection to mothers, especially single mothers.
7. To enable past, present, and future psychiatrists to provide quality mental healthcare to their patients.
8. Conclusions
The findings from the questionnaire survey, my extensive research, and my education and professional career have affirmed for me the relevance of Psychiatry and the need to improve access to mental healthcare to mitigate the widespread impact of our national mental health crisis. Achieving this need will require a cohesive, systemic approach from mental health providers to communities, institutions, and healthcare organizations. It is hoped that studies such as this, done across much larger samples, will provide the data and arguments needed to spark a cultural transformation that will reverse today's access issues.
Abbreviations
BIPOC | Black, Indigenous, and People of Color |
LGBTQIA+ | Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, Asexual, + (Other Sexual Identities) |
ACE | Adverse Childhood Experiences |
Author Contributions
Mercedes Agudo is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The author declares no conflicts of interest.
Appendix
Appendix I: Tables and Figures
Table 1. Demographic Characteristics Demographic characteristics of psychiatrists who responded to the survey.
CHARACTERISTICS | FREQUENCY (n = 48) | PERCENTAGES (%) |
GENDER | | |
Male | 24 | 50% |
Female | 24 | 50% |
EXTENT OF TIME SPENT AT | | |
WORK | | |
Full time | 36 | 75% |
Part time | 8 | 17% |
Retired | 4 | 8% |
AGE BRACKET IN YEARS | | |
30-34 | 1 | 2% |
35-39 | 2 | 4% |
40-44 | 2 | 4% |
45-49 | 5 | 10% |
50-54 | 6 | 13% |
55-59 | 8 | 17% |
60-64 | 3 | 6% |
65-69 | 9 | 19% |
70-74 | 5 | 10% |
75-79 | 5 | 10% |
80-84 | 1 | 2% |
85-89 | 1 | 2% |
YEARS OF PRACTICE AS | | |
PSYCHIATRIST | | |
0to4 | 4 | 8% |
5 to 9 | 4 | 8% |
10 to 14 | 5 | 10% |
15 to 19 | 2 | 4% |
20 to 24 | 4 | 8% |
25 to 29 | 9 | 20% |
30 to 34 | 5 | 10% |
35 to 39 | 2 | 4% |
40 to 44 | 7 | 15% |
45 to 49 | 4 | 8% |
50 to 54 | 1 | 2% |
55 to 59 | 1 | 2% |
Table 2. Factor Responses. Psychiatrists' responses to a brief survey pertaining to the above 7 factors rated in a 5-grid scale.
Factor | 1 Completely Disagree | 2 Partially Disagree | 3 Neutral | 4 Partially Agree | 5 Completely Agree |
1. Lack of support to mental health organizations | 4 (8%) | 1 (2%) | 9 (19%) | 21 (44%) | 14 (29%) |
2. Leadership problem or administration problem | 3 (6%) | 4 (8%) | 10 (21%) | 17 (35%) | 14 (29%) |
3. Shortage of psychiatrists | 0 (0%) | 1 (2%) | 8 (17%) | 22 (46%) | 17 (35%) |
4. Stigma in psychiatry and patients with mental illness | 1 (2%) | 2 (3%) | 9 (19%) | 25 (52%) | 11 (23%) |
5. Lack of support in training medical students, psychiatry residents and psychiatry fellows. | 3 (6%) | 6 (13%) | 10 (21%) | 22 (46%) | 7 (15%) |
6. Breakdown of family structure as, "Family is the cradle of good citizenship." | 3 (6%) | 12 (25%) | 10 (21%) | 11 (23%) | 12 (25%) |
7. Disparity in mental health care delivery | 1 (2%) | 3 (6%) | 4 (8%) | 13 (27%) | 27 (56%) |
Table 3. Factor Rankings Ranking of the 7 items by psychiatrists with number 1 as the most relevant factor to national mental health crisis and number 7 as the least relevant factor to national mental health crisis.
Factor | NUMBER of RANKINGS (Respondents asked to rank the factors by importance) |
#1 | #2 | #3 | #4 | #5 | #6 | #7 |
1. Lack of support to mental health organizations | 11 | 12 | 8 | 9 | 0 | 5 | 1 |
2. Leadership problem or administration problem | 4 | 12 | 6 | 6 | 6 | 4 | 8 |
3. Shortage of psychiatrists | 11 | 8 | 8 | 8 | 5 | 2 | 6 |
4. Stigma in psychiatry and patients with mental illness | 4 | 11 | 10 | 8 | 5 | 7 | 1 |
5. Lack of support in training medical student, psychiatry residents and psychiatry fellows. | 1 | 7 | 8 | 9 | 9 | 7 | 6 |
6. Breakdown of family structure as, "Family is the cradle of good citizenship." | 11 | 6 | 7 | 4 | 5 | 8 | 15 |
7. Disparity in mental health care delivery | 11 | 7 | 6 | 6 | 6 | 4 | 4 |
Table 4.
Questions addressed to immigrants | [45] | Rack P Migration and mental illness in Cox J Editor. Transcultural psychiatry. New Hampshire: Croom Helm Ltd. 1986. p. 59. |
Addressed to immigrants | Is the new culture valued and to be adopted? |
YES | NO |
Is the old culture valued and to be retained? | YES | INTEGRATION | SEPARATISM |
NO | ASSIMILATION | MARGINALITY |
Table 5.
Questions addressed to host communities | [45] | Rack P Migration and mental illness in Cox J Editor. Transcultural psychiatry. New Hampshire: Croom Helm Ltd. 1986. p. 59. |
Addressed to Host Communities | Are newcomers helped and encouraged to adopt the host culture and rewarded for doing so? |
YES | NO |
Are racial differences and alternative lifestyles respected? | YES | INTEGRATION | SEPARATION |
NO | ASSIMILATION | MARGINALITY |
Figure 2. Qualitative Data.
What is your motivation to keep your primary job?
Figure 3. Ranking of Factors.
Ranking of the seven item factors with the base as the least relevant to the top as the most relevant factor related to national mental health crisis.
Appendix II: Questionnaire/Survey
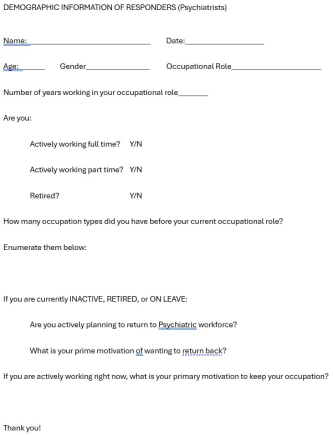
Figure 4. Demographic information of Psychiatrist respondents.
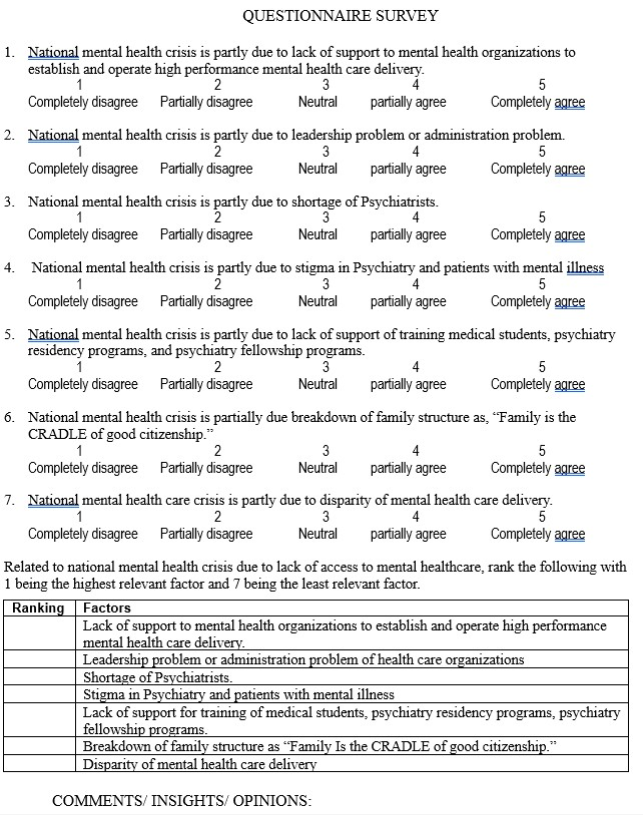
Figure 5. Questionnaire survey in Likert scale and ranking of the seven item factors contributing to accessibility issue of mental healthcare.
Appendix III: Research Poster
Figure 6. Research Poster to visualize a brief overview of the research.
Appendix IV: The Annual Cost of Untreated Mental Illness
References
| [1] |
Pollack, R. Foreword in Trevedi H., Sharfstein S. Editors. Textbook of hospital psychiatry. 2nd Ed. Washington, DC: American Psychiatric Association Publishing. 2023. p. xix.
|
| [2] |
Agudo M, Richie W. Panic disorder diagnosed as schizophrenia: a transcultural issue. National Medical Association. 100th Scientific Assembly. Annual Chester M. Pierce, MD, ScD Resident and Medical Student Symposium. 1995 July 31.
|
| [3] |
Wisner K, Murphy C, Thomas M. Prioritizing maternal mental health in addressing morbidity and mortality. JAMA Psychiatry. 2024; 8l (E2-E6).
|
| [4] |
Ehassan H, Robbins-Welty G, Moxley J. Geriatric psychiatrists' perspectives on palliative care: results from a national survey. Journal of Geriatric Psychiatry and Neurology. 2024; 37(1): 3-13.
|
| [5] |
Redd, K. "Suicide is a public health crisis". Native Americans disproportionately impacted by suicide. ABC lo+. 2023 March 24.
|
| [6] |
Weinstock, C. Native American communities have the highest suicide rates, yet interventions are scarce. CNN KFF Health News. 2024, January 26.
|
| [7] |
Wei, L, Woodruff A, et al Comment & response. Opioid use disorder treatment for patients who are incarcerated. JAMA. 2023; 330(13): 1284-5.
|
| [8] |
Strawbridge R, Graham N. Editorials. Dissecting the genetic relationship between schizophrenia and cardiovascular disease. Am Journal of Psychiatry. 2023; 180(11): 785-6.
|
| [9] |
Martins R, Kadakia A, Williams R, et al. The lifetime burden of schizophrenia as estimated by government-centric fiscal analytic: framework. J Clin Psychiatry. 2023; 84(5): 30-7.
|
| [10] |
Moukaddam, N. What happens to your psychiatric patient beyond the emergency department. Audio Digest. 2022 Sept 21; 51(18).
|
| [11] |
Meadows A, Strickland J, Haeder S. et al. Adverse childhood experiences and early initiation of substance use: A survival analysis. The International Journal of Psychiatry in Medicine. 2024; 59(2): 218-31.
|
| [12] |
Yatgur, B. Euthanasia for mental illness: right or wrong. Clinical Psychiatric News. 2023; 51(11): l.
|
| [13] |
Levounis P. In confronting addiction, older adults fall through the cracks. From the president. Psychiatric News. 2023; 58(10): 2.
|
| [14] |
Moran M. Levounis convenes medical leaders to collaborate on addiction. Psychiatric News. 2023; 58(10): l.
|
| [15] |
Ortega A., Roby D. Ending structural racism: US healthcare System to eliminate healthcare inequities. Department of Health Public Policy. JAMA 2021; 326(7): 613-15.
|
| [16] |
Mensah M, Owda D, Simons E, et al. Research letter US postgraduate trainee racial, ethnic, gender representation and faculty compensation by specialty. JAMA. 2023; 330(9): 872.
|
| [17] |
Da Silva F. Carvalho 0, Neto R. "COVID-19 and immunization: Reflections and rationale on why child and adolescent psychiatry should help. JMCAP. 2023; 62(5): 509- 11.
|
| [18] |
Brohan H, Chawdhary N, Dua T. The WHO Mental Health Gap Action Programme for mental, neurological, and substance use conditions: the new and updated guideline recommendations. The Lancet. 2023; 11: 155-58.
|
| [19] |
Cullen-Lester K, Maupin C, Carter D. Incorporating social networks into leadership development: a conceptual mode and evaluation of research and practice. The Leadership Quarterly. 2016; 28(1): 130-52.
|
| [20] |
Nayar V Employees First/Customers Second: Turning conventional leadership upside down. Harvard Business Press. 2010.
|
| [21] |
Maximo S. A scoping review of ethical consideration in spiritua1/religious counseling and psychotherapy. Journal of Pastoral Care & Counseling. 2019; 73(2): 123-133.
|
| [22] |
Kanter R. Why innovation is so hard in healthcare and how to do it anyway. Harvard Business Press. 2011 Feb 22.
|
| [23] |
Romanelli R; Marjanovick S. Diversity, equity, and inclusion in healthcare innovation: considerations for future research, policy and practice. Rand Corporation Blog. 2022 July 6.
|
| [24] |
Natterson-Horowitz, B. What scientists are learning about women's health from female animals. Scientific American. 2023 March.
|
| [25] |
Warshay, D. Chapter 3 Step 1 See: find and validate unmet needs. See, solve, scale: how anyone can turn an unsolved problem through success. 2022.
|
| [26] |
Luca, M. The two-parent privilege review: where have all good men gone? The Wall Street Journal. 2023 Sept 24.
|
| [27] |
McMillan K. I survived the foster care system. Dismantling it altogether is the only path forward. USA Today. 2023 Sept 24.
|
| [28] |
Hallett E, Simeon E, Amba V, et al. Factors influencing turnover and attrition in the public behavioral health system workforce: qualitative study. Psychiatric Services. 2024; 75(1): 55-63.
|
| [29] |
Abduhakimovna S. Social-psychological characteristics of the formation of family relations in adolescents. Journal of Child Psychology and Psychiatry. 2024; 7(1): 55-60.
|
| [30] |
Fagan J. The myth oflow-income black fathers' absence from the lives of adolescents. Journal of Family Issues. 2024; 45(1): 144-162.
|
| [31] |
Forsyth J, Bearden C. Rethinking the first episode of schizophrenia: identifying convergent mechanisms during development and moving toward prediction. AJP. 2023; 180(11): 792-804.
|
| [32] |
Ruiz-White I, Kramer L, Philips L. et al. Racial and ethnic disparities in physical and mental healthcare and clinical trials. J Clin Psychiatry. 2023; 84(4): 54-64.
|
| [33] |
Van der Ven E, Susser E. Structural racism and risk of schizophrenia. Am J Psychiatry. 2023; 180(11): 782-4.
|
| [34] |
Mercado, A, Boyd J, Chesky K. US medical student health insurance coverage for mental health treatment after the COVID 19 pandemic. JAMA Intern Med 2023; 183(11): 1273- 75.
|
| [35] |
Knaak S, Mantler E. Mental illness-related stigma in healthcare: barriers to access and care and evidenced based solutions. Healthcare Management Forum. 2017; 30: 111-6.
|
| [36] |
Khushalani S. Lean and Operational Excellence. Chapter 22 in Trevedi H, Sharfstein S, Editors. Textbook of Hospital Psychiatry. 2nd Ed. Washington, DC. American Psychiatric Association Publishing. c. 2023. p 505.
|
| [37] |
Brady K, Ni P, Lindsey P. et al. Establishing crosswalks between measures of burnout in US Physicians. Gen Internal Med. 2022; 37(4): 777-84.
|
| [38] |
Fawzi W, Partap U. Optimizing interventions from early development. JAMA. 2024; 331(1).
|
| [39] |
Bai G, Simon K, Cram P. Health equity measures and hospital rankings. JAMA. 2023; 329(9): 764.
|
| [40] |
Young A, Pei X, Arnhart K, et al. FSMB Census of licensed physicians in the United States, 2022. Journal of Medical Regulation. 2023; 109(2): 13-20.
|
| [41] |
Greenlaw, S, Shapiro D. Principles of Microeconomics. AnnArbor (MI): Rice University OpenStax.2018. p. 83.
|
| [42] |
Bullepalli H, Evans R, Ludford S, et al. Burnout among surgeons: lessons for psychiatrists. Current Psychiatry. 2023; 22(8): 23-35.
|
| [43] |
Sharma N, Sargent J. Chapter 9 in Parekh R, Al-Mateen C, Lisotto M et al Editors. Cultural psychiatry with children, adolescents, and families. Washington (DC): First Edition. American Psychiatric Association Publishing. 2021. pp 151-152.
|
| [44] |
Austin J, Bentkover J, Chait L. Leading strategic change in anera of healthcare transformation. Providence (RI): Springer International Publishing Switzerland. 2016. p. 61.
|
| [45] |
Rack P Migration and mental illness in Cox J Editor. Transcultural psychiatry. New Hampshire: Croom Helm Ltd. 1986. p. 59.
|
| [46] |
Valant Medical Solutions. The cost of untreated mental illness. 2017 Jan 26. Available from:
https://www.valant.io/resources/blog/the-cost-of-untreated-mental-illness/
|
Cite This Article
-
APA Style
Agudo, M. (2025). Psychiatry: The Relevance of Improving Access to Healthcare for Acutely Mentally Ill and Those with Longstanding Mental Illness. American Journal of Psychiatry and Neuroscience, 13(2), 36-49. https://doi.org/10.11648/j.ajpn.20251302.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Agudo, M. Psychiatry: The Relevance of Improving Access to Healthcare for Acutely Mentally Ill and Those with Longstanding Mental Illness. Am. J. Psychiatry Neurosci. 2025, 13(2), 36-49. doi: 10.11648/j.ajpn.20251302.11
Copy
|
Download
AMA Style
Agudo M. Psychiatry: The Relevance of Improving Access to Healthcare for Acutely Mentally Ill and Those with Longstanding Mental Illness. Am J Psychiatry Neurosci. 2025;13(2):36-49. doi: 10.11648/j.ajpn.20251302.11
Copy
|
Download
-
@article{10.11648/j.ajpn.20251302.11,
author = {Mercedes Agudo},
title = {Psychiatry: The Relevance of Improving Access to Healthcare for Acutely Mentally Ill and Those with Longstanding Mental Illness
},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {13},
number = {2},
pages = {36-49},
doi = {10.11648/j.ajpn.20251302.11},
url = {https://doi.org/10.11648/j.ajpn.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20251302.11},
abstract = {Background: There is currently a national mental health crisis due to the lack of access to mental health care. Objectives: 1. To study the different factors that contribute to lack of access to psychiatric treatment. 2. To compare each factor by ranking them according to their relevance in contributing to the lack of access to health care and national mental health crisis as perceived by psychiatrist respondents to a brief survey. 3. To analyze results, discuss implications, and provide recommendations. Methods: Seven factors contributing to lack of access to psychiatric treatment are identified from a review of literature, educational materials, and clinical practice. A cross-sectional survey of psychiatrists in US practice is conducted from July to December 2023 by convenient sampling. Recruitment is done in person and via email, US postal mail, and telephone. Forty-eight respondents rated these factors in a Likert scale and ranked them, taking 15 minutes to complete each survey. Quantitative data are analyzed descriptively, and qualitative data are analyzed deductively by identifying the themes from respondents’ narratives. Results: The factors contributing to lack of access to psychiatric treatment are ranked as follows: 1. Lack of support to mental health organizations to establish and operate high-performance mental healthcare delivery (score: 11). 2. Leadership problem and administration problem (score: 12). 3. Stigma in psychiatrists and patients (score: 10) 4. Lack of support in training medical students (score: 9) 5. Disparity in mental healthcare delivery (score: 6) 6. Breakdown of family structure as, “Family is the cradle of good citizenship” (score: 8) 7. Shortage of psychiatrists (score: 6). The theme that emerged from respondents’ narratives about keeping their job are: 1. Enjoyment 2. Financial 3. Altruism 4. Structure. Conclusions: This study has affirmed the relevance of Psychiatry and the need to improve access to mental healthcare. This will require systemic approach from mental health providers to communities, institutions, and healthcare organizations. It is hoped that studies such as this will spark a cultural transformation that will reverse healthcare access issues.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Psychiatry: The Relevance of Improving Access to Healthcare for Acutely Mentally Ill and Those with Longstanding Mental Illness
AU - Mercedes Agudo
Y1 - 2025/04/22
PY - 2025
N1 - https://doi.org/10.11648/j.ajpn.20251302.11
DO - 10.11648/j.ajpn.20251302.11
T2 - American Journal of Psychiatry and Neuroscience
JF - American Journal of Psychiatry and Neuroscience
JO - American Journal of Psychiatry and Neuroscience
SP - 36
EP - 49
PB - Science Publishing Group
SN - 2330-426X
UR - https://doi.org/10.11648/j.ajpn.20251302.11
AB - Background: There is currently a national mental health crisis due to the lack of access to mental health care. Objectives: 1. To study the different factors that contribute to lack of access to psychiatric treatment. 2. To compare each factor by ranking them according to their relevance in contributing to the lack of access to health care and national mental health crisis as perceived by psychiatrist respondents to a brief survey. 3. To analyze results, discuss implications, and provide recommendations. Methods: Seven factors contributing to lack of access to psychiatric treatment are identified from a review of literature, educational materials, and clinical practice. A cross-sectional survey of psychiatrists in US practice is conducted from July to December 2023 by convenient sampling. Recruitment is done in person and via email, US postal mail, and telephone. Forty-eight respondents rated these factors in a Likert scale and ranked them, taking 15 minutes to complete each survey. Quantitative data are analyzed descriptively, and qualitative data are analyzed deductively by identifying the themes from respondents’ narratives. Results: The factors contributing to lack of access to psychiatric treatment are ranked as follows: 1. Lack of support to mental health organizations to establish and operate high-performance mental healthcare delivery (score: 11). 2. Leadership problem and administration problem (score: 12). 3. Stigma in psychiatrists and patients (score: 10) 4. Lack of support in training medical students (score: 9) 5. Disparity in mental healthcare delivery (score: 6) 6. Breakdown of family structure as, “Family is the cradle of good citizenship” (score: 8) 7. Shortage of psychiatrists (score: 6). The theme that emerged from respondents’ narratives about keeping their job are: 1. Enjoyment 2. Financial 3. Altruism 4. Structure. Conclusions: This study has affirmed the relevance of Psychiatry and the need to improve access to mental healthcare. This will require systemic approach from mental health providers to communities, institutions, and healthcare organizations. It is hoped that studies such as this will spark a cultural transformation that will reverse healthcare access issues.
VL - 13
IS - 2
ER -
Copy
|
Download