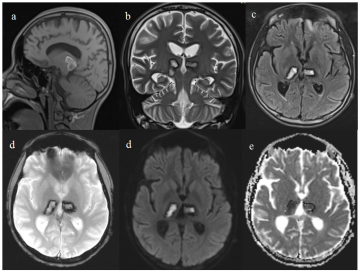
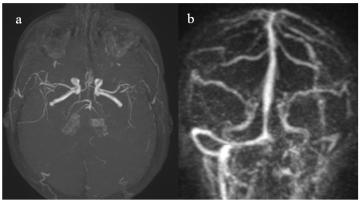
Cerebral venous thrombosis (CVT) constitutes less than 1% of stroke occurrences. The prevalence of abnormal movements following a stroke remains unclear, with movement disorders observed after a stroke ranging from 13 to 22% of secondary disorders. Nonetheless, these disorders are present in only 1% to 4% of stroke cases, with dystonias being the most commonly linked abnormalities in ischemic strokes. The lesions that lead to dystonias primarily affect the basal ganglia, thalamus, brainstem, cerebellum, and specific cortical regions. Dystonias make up about 30% of abnormal movements observed after a thalamic stroke, with the lesions typically being unilateral. This research discusses instances of delayed paroxysmal dystonias related to bilateral hemorrhagic infarction in the thalamus of an adolescent with cerebral venous thrombosis. A 15-year-old adolescent was admitted due to a rapidly developing disturbance of consciousness. Upon arrival, he exhibited a non-massive left hemicorporal pyramidal syndrome, left-sided tonic seizures, and a state of confusion. Magnetic resonance imaging revealed a bilateral thalamic hemorrhagic focus and cerebral venous thrombosis. Anticoagulant therapy was initiated, and the clinical progression during the acute phase was satisfactory. Ten days later, the patient displayed generalized but asymmetrical paroxysmal dystonias, predominantly affecting the left hemibody. This case presented diagnostic challenges, as the abnormal dystonic movements were linked to focal tonic seizures, alongside management issues, given that most antidystonic medications are sedative in nature, complicating treatment due to the pre-existing disturbance of consciousness. Nevertheless, the patient's condition improved under cautious administration of anticholinergic agents and GABAergic agonists.
| Published in | American Journal of Psychiatry and Neuroscience (Volume 13, Issue 1) |
| DOI | 10.11648/j.ajpn.20251301.11 |
| Page(s) | 1-6 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Paroxysmal Dystonia, Cerebral Venous Thrombosis, Thalamic Venous Infarct, Adolescent, Management
GCS | Glasgow Coma Scale |
MRI | Magnetic Resonance Imaging |
FLAIR | Fluid-Attenuated Inversion Recovery |
ADC | Apparent Diffusion Coefficient |
MIP | Maximum Intensity Projection |
BoNT | Botulinum Neurotoxins |
GABA | Gamma-Aminobutyric Acid |
| [1] | J. Phukan, A. Albanese, T. Gasser, and T. Warner, “Primary dystonia and dystonia-plus syndromes: clinical characteristics, diagnosis, and pathogenesis,” The Lancet Neurology, vol. 10, no. 12, pp. 1074–1085, Dec. 2011, |
| [2] | K. Grütz and C. Klein, “Dystonia updates: definition, nomenclature, clinical classification, and etiology,” J Neural Transm (Vienna), vol. 128, no. 4, pp. 395–404, Apr. 2021, |
| [3] | S. A. Schneider and K. P. Bhatia, “Secondary Dystonia-Clinical Clues and Syndromic Associations,” J Mov Disord, vol. 2, no. 2, pp. 58–63, Oct. 2009, |
| [4] | R. Suri et al., “Post-stroke Movement Disorders: The Clinical, Neuroanatomic, and Demographic Portrait of 284 Published Cases,” J Stroke Cerebrovasc Dis, vol. 27, no. 9, pp. 2388–2397, Sep. 2018, |
| [5] | P. Krystkowiak, P. Martinat, L. Defebvre, J. P. Pruvo, D. Leys, and A. Destée, “Dystonia after striatopallidal and thalamic stroke: clinicoradiological correlations and pathophysiological mechanisms,” J Neurol Neurosurg Psychiatry, vol. 65, no. 5, pp. 703–708, Nov. 1998, |
| [6] | S. Lehéricy et al., “Striatopallidal and thalamic dystonia. A magnetic resonance imaging anatomoclinical study,” Arch Neurol, vol. 53, no. 3, pp. 241–250, Mar. 1996, |
| [7] | H. R. Alvis-Miranda, S. Milena Castellar-Leones, G. Alcala-Cerra, and L. Rafael Moscote-Salazar, “Cerebral sinus venous thrombosis,” J Neurosci Rural Pract, vol. 4, no. 4, pp. 427–438, 2013, |
| [8] | G. C. Magala et al., “Cerebral venous thrombosis as an uncommon etiology of spontaneous subarachnoid hemorrhage: Case report,” J Clin Images Med Case, vol. Volume 5, no. 9, http://www.doi.org/10.52768/2766-7820/3270 |
| [9] | L. Ulivi, M. Squitieri, H. Cohen, P. Cowley, and D. J. Werring, “Cerebral venous thrombosis: a practical guide,” Practical Neurology, vol. 20, no. 5, pp. 356–367, Oct. 2020, |
| [10] | J. L. Leach, R. B. Fortuna, B. V. Jones, and M. F. Gaskill-Shipley, “Imaging of cerebral venous thrombosis: current techniques, spectrum of findings, and diagnostic pitfalls,” Radiographics, vol. 26 Suppl 1, pp. S19-41; discussion S42-43, Oct. 2006, |
| [11] | A. Siniscalchi, L. Gallelli, A. Labate, G. Malferrari, C. Palleria, and G. D. Sarro, “Post-stroke Movement Disorders: Clinical Manifestations and Pharmacological Management,” Curr Neuropharmacol, vol. 10, no. 3, pp. 254–262, Sep. 2012, |
| [12] | F. Ghika-Schmid, J. Ghika, F. Regli, and J. Bogousslavsky, “Hyperkinetic movement disorders during and after acute stroke: the Lausanne Stroke Registry,” J Neurol Sci, vol. 146, no. 2, pp. 109–116, Mar. 1997, |
| [13] | A. Albanese et al., “Phenomenology and classification of dystonia: a consensus update,” Mov Disord, vol. 28, no. 7, pp. 863–873, Jun. 2013, |
| [14] | N. Gupta and S. Pandey, “Post-Thalamic Stroke Movement Disorders: A Systematic Review,” Eur Neurol, vol. 79, no. 5–6, pp. 303–314, 2018, |
| [15] | V. K. Neychev, X. Fan, V. I. Mitev, E. J. Hess, and H. A. Jinnah, “The basal ganglia and cerebellum interact in the expression of dystonic movement,” Brain, vol. 131, no. Pt 9, pp. 2499–2509, Sep. 2008, |
| [16] | H. A. Jinnah, “Diagnosis & Treatment of Dystonia,” Neurol Clin, vol. 33, no. 1, pp. 77–100, Feb. 2015, |
| [17] | A. Albanese et al., “EFNS guidelines on diagnosis and treatment of primary dystonias,” Eur J Neurol, vol. 18, no. 1, pp. 5–18, Jan. 2011, |
| [18] | A. Albanese et al., “A systematic review on the diagnosis and treatment of primary (idiopathic) dystonia and dystonia plus syndromes: report of an EFNS/MDS-ES Task Force,” Eur J Neurol, vol. 13, no. 5, pp. 433–444, May 2006, |
| [19] | R. E. Burke, S. Fahn, and C. D. Marsden, “Torsion dystonia: a double-blind, prospective trial of high-dosage trihexyphenidyl,” Neurology, vol. 36, no. 2, pp. 160–164, Feb. 1986, |
| [20] | T. D. Sanger et al., “Prospective open-label clinical trial of trihexyphenidyl in children with secondary dystonia due to cerebral palsy,” J Child Neurol, vol. 22, no. 5, pp. 530–537, May 2007, |
| [21] | P. Greene, “Baclofen in the treatment of dystonia,” Clin Neuropharmacol, vol. 15, no. 4, pp. 276–288, Aug. 1992, |
APA Style
Magala, G. C., Tanoh, A. C., Agbo-Panzo, S. A. C., Amon-Tanoh, M., Souza, A. N. T. E. D., et al. (2025). Challenges in Diagnosing and Managing Delayed Onset Paroxysmal Generalized Dystonias Associated with Bilateral Thalamic Hemorrhagic Venous Infarction Due to Extensive Cerebral Venous Thrombosis (CVT) in a 15-Year-Old Adolescent: A Case Study. American Journal of Psychiatry and Neuroscience, 13(1), 1-6. https://doi.org/10.11648/j.ajpn.20251301.11
ACS Style
Magala, G. C.; Tanoh, A. C.; Agbo-Panzo, S. A. C.; Amon-Tanoh, M.; Souza, A. N. T. E. D., et al. Challenges in Diagnosing and Managing Delayed Onset Paroxysmal Generalized Dystonias Associated with Bilateral Thalamic Hemorrhagic Venous Infarction Due to Extensive Cerebral Venous Thrombosis (CVT) in a 15-Year-Old Adolescent: A Case Study. Am. J. Psychiatry Neurosci. 2025, 13(1), 1-6. doi: 10.11648/j.ajpn.20251301.11
AMA Style
Magala GC, Tanoh AC, Agbo-Panzo SAC, Amon-Tanoh M, Souza ANTED, et al. Challenges in Diagnosing and Managing Delayed Onset Paroxysmal Generalized Dystonias Associated with Bilateral Thalamic Hemorrhagic Venous Infarction Due to Extensive Cerebral Venous Thrombosis (CVT) in a 15-Year-Old Adolescent: A Case Study. Am J Psychiatry Neurosci. 2025;13(1):1-6. doi: 10.11648/j.ajpn.20251301.11
@article{10.11648/j.ajpn.20251301.11,
author = {Gloire Chubaka Magala and Abel Christian Tanoh and Segla Achi Cedric Agbo-Panzo and Muriel Amon-Tanoh and Ahya Nancy Tanya Essoin De Souza and Fiacre Delors Offoumou and Arlette Désirée Aka and Roseline Mohou Felandine Kouassi and Léonard Kouamé Kouassi and Évelyne Aka-Anghui Diarra},
title = {Challenges in Diagnosing and Managing Delayed Onset Paroxysmal Generalized Dystonias Associated with Bilateral Thalamic Hemorrhagic Venous Infarction Due to Extensive Cerebral Venous Thrombosis (CVT) in a 15-Year-Old Adolescent: A Case Study
},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {13},
number = {1},
pages = {1-6},
doi = {10.11648/j.ajpn.20251301.11},
url = {https://doi.org/10.11648/j.ajpn.20251301.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20251301.11},
abstract = {Cerebral venous thrombosis (CVT) constitutes less than 1% of stroke occurrences. The prevalence of abnormal movements following a stroke remains unclear, with movement disorders observed after a stroke ranging from 13 to 22% of secondary disorders. Nonetheless, these disorders are present in only 1% to 4% of stroke cases, with dystonias being the most commonly linked abnormalities in ischemic strokes. The lesions that lead to dystonias primarily affect the basal ganglia, thalamus, brainstem, cerebellum, and specific cortical regions. Dystonias make up about 30% of abnormal movements observed after a thalamic stroke, with the lesions typically being unilateral. This research discusses instances of delayed paroxysmal dystonias related to bilateral hemorrhagic infarction in the thalamus of an adolescent with cerebral venous thrombosis. A 15-year-old adolescent was admitted due to a rapidly developing disturbance of consciousness. Upon arrival, he exhibited a non-massive left hemicorporal pyramidal syndrome, left-sided tonic seizures, and a state of confusion. Magnetic resonance imaging revealed a bilateral thalamic hemorrhagic focus and cerebral venous thrombosis. Anticoagulant therapy was initiated, and the clinical progression during the acute phase was satisfactory. Ten days later, the patient displayed generalized but asymmetrical paroxysmal dystonias, predominantly affecting the left hemibody. This case presented diagnostic challenges, as the abnormal dystonic movements were linked to focal tonic seizures, alongside management issues, given that most antidystonic medications are sedative in nature, complicating treatment due to the pre-existing disturbance of consciousness. Nevertheless, the patient's condition improved under cautious administration of anticholinergic agents and GABAergic agonists.
},
year = {2025}
}
TY - JOUR T1 - Challenges in Diagnosing and Managing Delayed Onset Paroxysmal Generalized Dystonias Associated with Bilateral Thalamic Hemorrhagic Venous Infarction Due to Extensive Cerebral Venous Thrombosis (CVT) in a 15-Year-Old Adolescent: A Case Study AU - Gloire Chubaka Magala AU - Abel Christian Tanoh AU - Segla Achi Cedric Agbo-Panzo AU - Muriel Amon-Tanoh AU - Ahya Nancy Tanya Essoin De Souza AU - Fiacre Delors Offoumou AU - Arlette Désirée Aka AU - Roseline Mohou Felandine Kouassi AU - Léonard Kouamé Kouassi AU - Évelyne Aka-Anghui Diarra Y1 - 2025/01/09 PY - 2025 N1 - https://doi.org/10.11648/j.ajpn.20251301.11 DO - 10.11648/j.ajpn.20251301.11 T2 - American Journal of Psychiatry and Neuroscience JF - American Journal of Psychiatry and Neuroscience JO - American Journal of Psychiatry and Neuroscience SP - 1 EP - 6 PB - Science Publishing Group SN - 2330-426X UR - https://doi.org/10.11648/j.ajpn.20251301.11 AB - Cerebral venous thrombosis (CVT) constitutes less than 1% of stroke occurrences. The prevalence of abnormal movements following a stroke remains unclear, with movement disorders observed after a stroke ranging from 13 to 22% of secondary disorders. Nonetheless, these disorders are present in only 1% to 4% of stroke cases, with dystonias being the most commonly linked abnormalities in ischemic strokes. The lesions that lead to dystonias primarily affect the basal ganglia, thalamus, brainstem, cerebellum, and specific cortical regions. Dystonias make up about 30% of abnormal movements observed after a thalamic stroke, with the lesions typically being unilateral. This research discusses instances of delayed paroxysmal dystonias related to bilateral hemorrhagic infarction in the thalamus of an adolescent with cerebral venous thrombosis. A 15-year-old adolescent was admitted due to a rapidly developing disturbance of consciousness. Upon arrival, he exhibited a non-massive left hemicorporal pyramidal syndrome, left-sided tonic seizures, and a state of confusion. Magnetic resonance imaging revealed a bilateral thalamic hemorrhagic focus and cerebral venous thrombosis. Anticoagulant therapy was initiated, and the clinical progression during the acute phase was satisfactory. Ten days later, the patient displayed generalized but asymmetrical paroxysmal dystonias, predominantly affecting the left hemibody. This case presented diagnostic challenges, as the abnormal dystonic movements were linked to focal tonic seizures, alongside management issues, given that most antidystonic medications are sedative in nature, complicating treatment due to the pre-existing disturbance of consciousness. Nevertheless, the patient's condition improved under cautious administration of anticholinergic agents and GABAergic agonists. VL - 13 IS - 1 ER -
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast
Research Fields: Cerebrovascular diseases, Neuroradiology, Neuroepidemiology, General Neurology
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast; Nervous System and Rehabilitation Department, Felix Houphouet-Boigny University, Abidjan, Ivory Coast
Research Fields: Neuroepidemiology, Neuroinfectiology, General Neurology, Neuro-degenerative diseases
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast; Nervous System and Rehabilitation Department, Felix Houphouet-Boigny University, Abidjan, Ivory Coast
Research Fields: General Neurology, epileptology, movements disorders
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast; Nervous System and Rehabilitation Department, Felix Houphouet-Boigny University, Abidjan, Ivory Coast
Research Fields: General Neurology, Cerebrovascular pathologies, fundamental Neu-rosciences
Nervous System and Rehabilitation Department, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Neurology Department, Yopougon Teaching Hospital, Abidjan, Ivory Coast
Research Fields: Child Neurology, epileptology, General Neurology
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast
Research Fields: General Neurology, Peripheral neurological disorders and muscle pathologies
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast
Research Fields: Epileptology, General Neurology
Psychiatry Department, Adjamé National Public Health Institute, Abidjan, Ivory Coast
Research Fields: Neurofonctionnal disorders, psychiatry
Nervous System and Rehabilitation Department, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Neurology Department, Yopougon Teaching Hospital, Abidjan, Ivory Coast
Research Fields: Neuropsychology and Neurodegenerative diseases, general Neurol-ogy
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast; Nervous System and Rehabilitation Department, Felix Houphouet-Boigny University, Abidjan, Ivory Coast
Research Fields: Epileptology, Peripheral neurological disorders, Neurophysiology, movement disorders, Epileptology